IPD or “integrated project delivery” is fast becoming the newest buzzword in the AEC industry after BIM, which has moved on from dominating the industry discourse for the last five years to becoming almost as commonplace as the term CAD. IPD, on the other hand, is a term that started being widely used only last year and is rapidly gaining in momentum, to the extent that it is now becoming a focal point of many AEC vendors’ product pitches. A case in point was the article on “Collaboration, Project Management, and Project Information Management Solutions in AEC” that was published last month, in which two of the three solutions profiled—Newforma and Attolist—had IPD listed as a critical component of their offerings. And Kalexo, a brand new collaboration offering that has just been launched, even has IPD right there in its tag line—“integrated project delivery platform for design, engineering, architecture, and construction.”
The IPD concept has been inspired by various alternate delivery models for building projecta that have been explored in different parts of the world, most notably the Project Alliance method that has been successfully implemented in Australia on 30 to 40 projects in the last few years. It was described in some detail at a presentation at the AIA Integrated Practice 2006 conference by Tony Rinella of Anshen+Allen and Jim Bedrick of Webcor Builders. While there is no official definition of IPD yet, I did find a good working definition in this 2007 document from the AIA California Council:
“Integrated Project Delivery (IPD) is a project delivery approach that integrates people, systems, business structures and practices into a process that collaboratively harnesses the talents and insights of all participants to reduce waste and optimize efficiency through all phases of design, fabrication and construction. IPD principles can be applied to a variety of contractual arrangements and IPD teams will usually include members well beyond the basic triad of owner, designer and contractor. At a minimum, though, an integrated project includes tight collaboration between the owner, architect/engineers, and builders ultimately responsible for construction of the project, from early design through project handover.”
While IPD is still more of a goal than a reality at the moment for most of the AEC industry, there are a few ground-breaking projects that are already using this new collaboration and delivery method. At Autodesk University in November (see AECbytes Newsletter #38), we heard about Autodesk’s own AEC headquarters in Waltham, MA, remodeled from an existing building, that was being implemented as an IPD project jointly with the architect (KlingStubbins) and contractor (Tocci Building Companies). I recently had the opportunity to learn about one more IPD project—the Sutter Medical Center Castro Valley (SMCCV) in California—which, being a hospital building, is much larger in size and scope. I even got some first-hand experience of how the IPD process works by attending one of the collaborative review meetings for the project. This article provides an overview of the SMCCV project and explores how the IPD approach is being used for it.
The SMCCV is a new, state-of-the-art 130-bed hospital, which will replace the current Eden Medical Center in Castro Valley, California. The vision was to create a landmark medical center that integrates advanced technology, quality medical care, and outstanding physicians and employees to provide the best care for patients and community. It is a $320 million project that is fully funded by Sutter Health, making it the first, comprehensive hospital rebuilding plan in its county that is financed without taxpayer support or public funds. Sutter Health is one of the nation’s leading not-for-profit networks of community-based health care providers, with over 60 facilities in Northern California including hospitals, cancer centers, long-term care centers, research institutes, and home health and hospice centers. Some rendered images of the new hospital project can be seen in Figure 1.

In addition to the construction of the new hospital building, the project also includes campus improvements including additional parking and the demolition of the old hospital once the new hospital is complete. The need for a new hospital arose from California’s hospital seismic safety law, SB1953, passed in 1994, that requires every hospital in the state to meet specific criteria that would keep these structures standing and provide uninterrupted care if they were struck by a major earthquake. The deadline for complying with SB1953 is by 2013. Under the stringent earthquake safety requirements, the original hospital building built in 1954 would not be eligible to be licensed as an acute care hospital after January 1, 2013. The hospital management and Sutter Health took advantage of this opportunity to not only build a safe and secure structure, but to also try and build an innovative, state-of-the-art hospital and deliver a new kind of health care. More information about the project and its continuing progress can be found at http://suttermedicalcentercastrovalley.org/blog/.
The new seismic safety law has mandated seismic improvements for many of other Sutter facilities as well, requiring the organization to execute several large projects within a specific time frame. This motivated Sutter to find ways to reduce the time delays and budget over-runs typically associated with large projects, as well as the extended litigation that often results. It was looking at ways by which the design and construction delivery model could be transformed, and IPD fortuitously emerged as a viable alternative to the traditional delivery model just as the SMCCV project was being initiated. Moreover, the SMCCV project had several additional challenges that made it a good candidate for IPD: it had hard deadlines for both design and construction, an accelerated schedule that was 30% faster than a conventional schedule, and an aggressive cost target that could not be exceeded. None of these could be met with the conventional design-bid-build process, as that is iterative and takes too long, and any attempt to fast track the process usually results in higher risk of rework or cost increases. The IPD approach was therefore adopted for this project, in conjunction with the principles of lean construction and the implementation of technologies such as BIM.
The core team was assembled early on in the planning process, and they have signed a preliminary IFOA (Integrated Form of Agreement) that commits them to function as an IPD team. The team includes the following 10 parties:
GHAFARI is a leading A/E firm noted for its use of advanced AEC technologies, as described in my 2005 feature, “Multi-Disciplinary BIM at Work at GHAFARI Associates,” and it regularly leverages its expertise in the form of consulting services outside of its own commissioned projects. The architectural firm, Devenney Group, is a leader in healthcare design, with over a 100 trained staff members currently working on healthcare projects in Texas and California, and uses BIM extensively along with supporting collaboration and analysis tools. Another firm on the SMCCV team that ranks high on advanced technology adoption is DPR Construction, which also has a history of working on other Sutter Health projects using the principles of lean construction. The other firms on the team also have a fair amount of experience working with BIM. All in all, it is a solid team for what is going to be one of the early large-scale IPD projects in the US.
The preliminary IFOA does not include the Estimated Maximum Price (the IFOA equivalent of the conventional Guaranteed Maximum Price or GMP). However, this will be included in the final contract along with profit-sharing incentives for all the participating firms to finish the project on time and under budget. That full contract is expected to be negotiated and signed closer to the start of construction later on this summer. The IPD approach has encouraged the participating firms to change their normal work process and devote people full-time to this project, as opposed to the traditional process where they typically have people working on 3 to 4 projects at a time. In addition to the core IPD team, there are over 25 additional firms in the expanded project team, who are also supporting the IPD approach and adjusting their traditional processes to work with it.
An important aspect of meeting the time deadline for this project was to improve upon the typical review process by the state regulatory agency for hospitals, OSHPD (Office of Statewide Health Planning & Development). This agency normally takes 16-24 months to review a conventionally designed project after it has been submitted and issue the necessary approvals and permit. The IPD team for the SMCCV project is using a “phased review” approach instead, where they submit the fully coordinated construction documents to OSHPD in stages (see Figure 2). The final document set including the structural package was submitted in December 2008, and the initial permit is expected to be received in June, allowing the foundation work to start in July or August, while the rest of the project is being reviewed by OSHPD. The construction should end by May or June of 2012, allowing at least six months for licensing and move in by the hard deadline of December 2012.
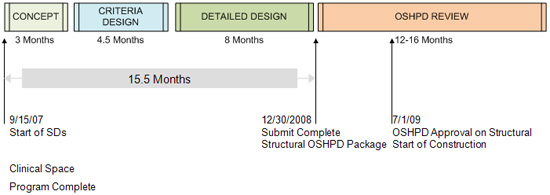
In reality, the clinical program took longer to finalize than the date shown in the above schedule, as it was more complex than had been anticipated. Since the program is the fundamental decision that drives everything else, the project team and management decided to allow as much thoughtful deliberation as possible to go into that decision. But the design was still able to be completed on time, thanks to the IPD approach and the tools and strategies that will be described in the next section. The reduction in design time also had the advantage of reducing costs, as the billable hours were very low for that additional time period that was taken to finalize the clinical program.
Given the challenges of the site, the complicated shape of the design, and the schedule and budget constraints, the use of BIM on this project was indispensable (see Figure 3). The approach was to produce a multi-disciplinary, fully coordinated 3D model first, delay the production of paper documents until the last responsible moment, and then produce them with as little rework as possible. The team was also determined to use direct digital exchange to the fullest extent possible, re-using the design model for estimation as well as for fabrication. Other strategies were to eliminate arbitrary gates and handoffs, allowing information to smoothly flow into downstream processes; enable early and direct input on the design from the fabricators to increase fabrication and pre-assembly efficiencies; and allow real-time access to all project information regardless of its authoring location, quantity, or file size by implementing Bentley’s ProjectWise information management and document control application.
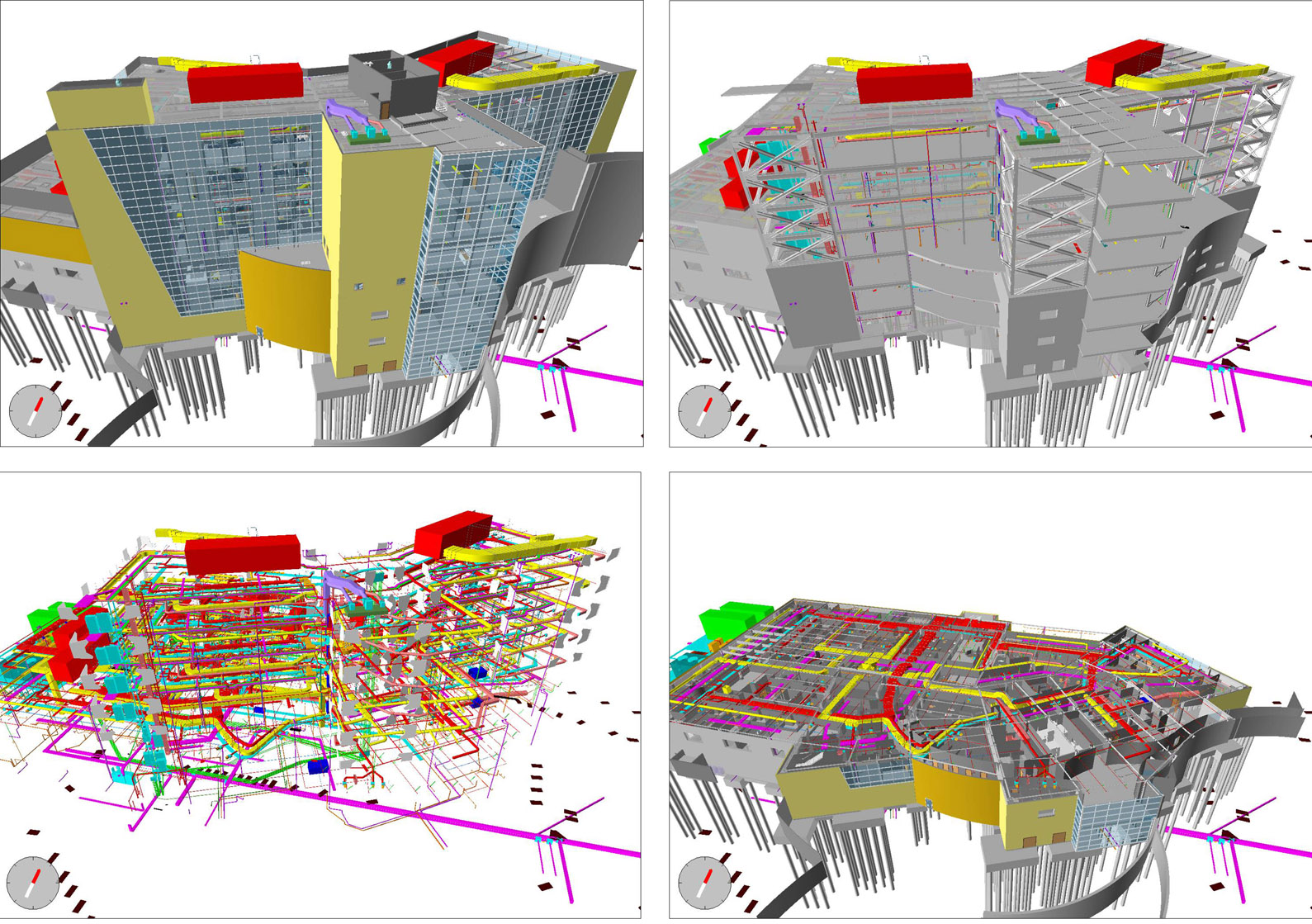
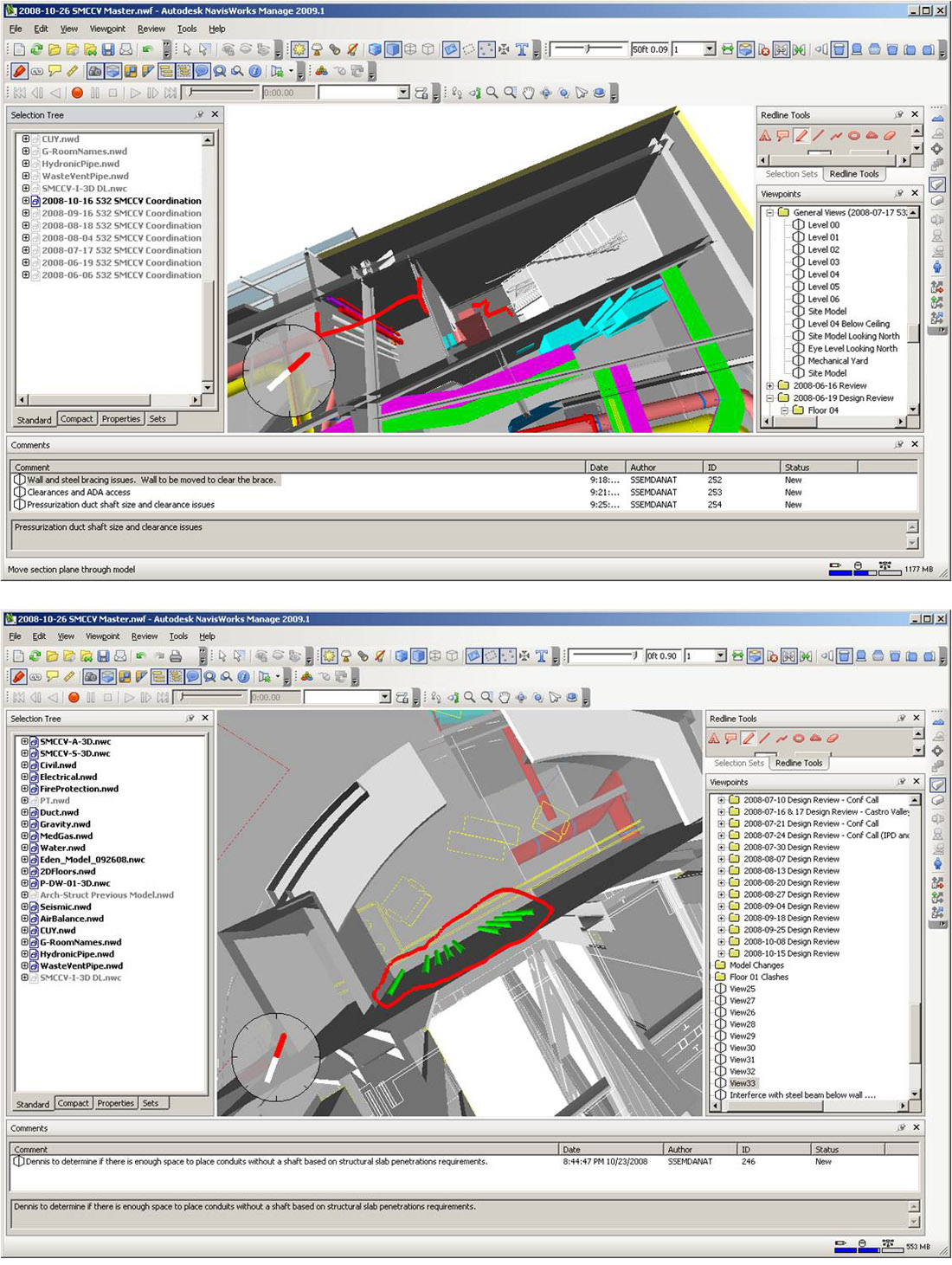
With regard to BIM, all the firms are using the solutions that they have expertise in. The main design applications are Revit Architecture; Revit Structure; CAD-Mech, CAD-Duct and CAD-pipe from TSI, which are AutoCAD-based HVAC programs; and AutoCAD MEP for electrical engineering and seismic restraint. In addition, Tekla Structures is being used by the structural fabricator and CAD Sprink by the fire sprinkler designer. Many of the models are being collaboratively developed, for example, the MEP engineer and detailer are working in sync on the same model, and so are the architect and contractor, with help from the GHAFARI consulting team. Continuous design reviews of the 3D models using NavisWorks are allowing the cross-functional team to contribute their best practices and iterate through the design more frequently early in the process to arrive at better solutions (see Figure 4).
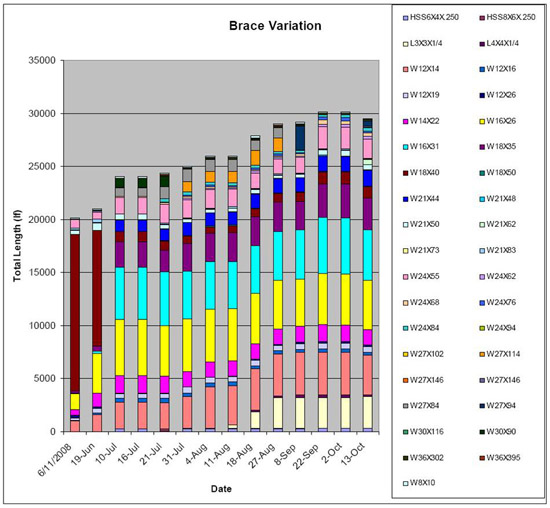
The reliability of the information in the models is enabling the team to extract automated quantity takeoffs frequently and more accurately (see Figure 5). The GC for the project, DPR Construction, is taking the lead on using model-based estimating for the architectural and structural elements. Estimating is done more often and in less time as the design evolves and quantities are further detailed and refined. However, the team also did realize that model-based estimating is not as easy as is generally advertised. To get a detailed and accurate estimate from the model, time needs to be spent upfront deciding who is going to model what, so that there are no overlaps. Also, model-based estimating has not worked as successfully yet for the MEP elements, and the team is continuing to work on resolving that in collaboration with the MEP software vendor, TSI.
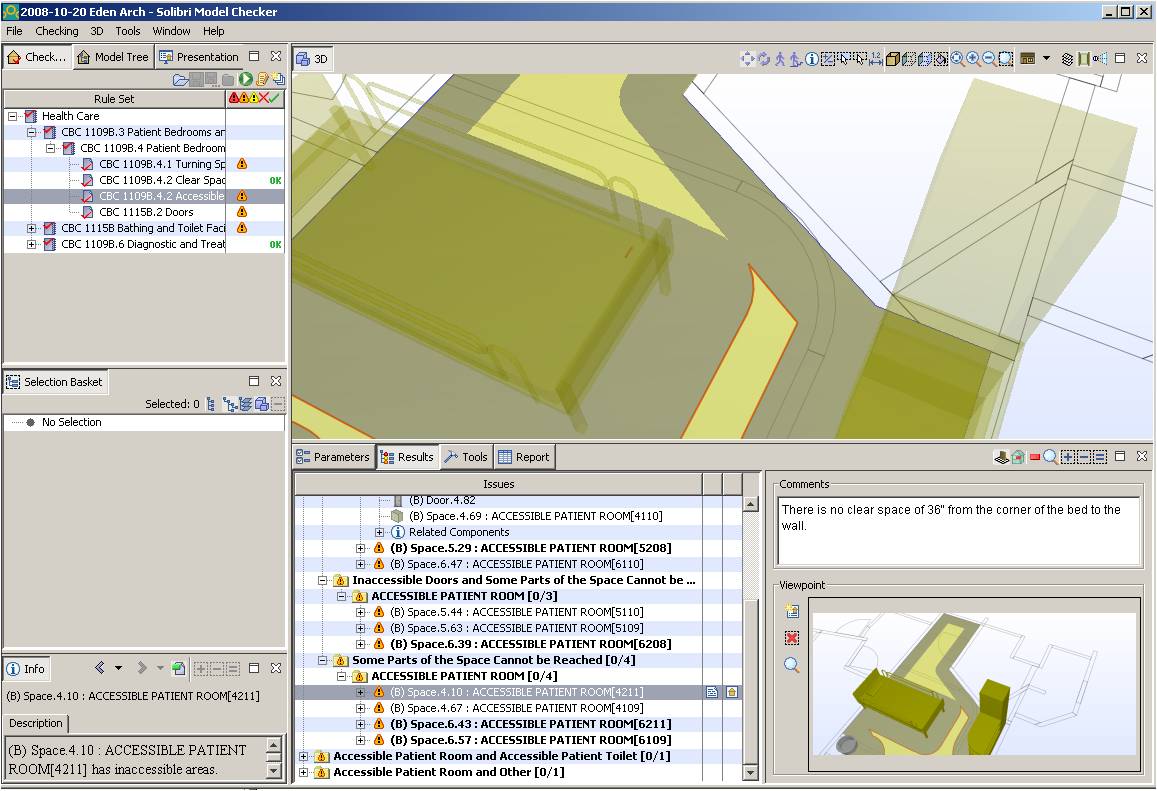
Another use of the model that is being explored is automated code-checking using Solibri Model Checker, as shown in Figure 6. This is being done as early in the design stages as possible so that the results can be used to spot problems with the design early on. The SMCCV IPD team finds this area very promising, even though the technology still needs a great deal of development to make it more usable and effective.
One especially noteworthy aspect of the SMCCV project is the extensive use of a technique originally developed by Toyota called Value Stream Mapping (VSM). It is a visual method of documenting workflow to identify value added and non-value added supply chain actions required to deliver a product to a customer, allowing the most effective material/information flows to be chosen for maximizing value and eliminating waste. While it originated in manufacturing, VSM is also used in logistics, supply chain, service related industries, healthcare, software development, and product development. The SMCCV team is using it to continuously improve their design process and streamline workflows, and have been able to achieve substantial design time savings because of it. Some examples of the maps at various stages are shown in Figure 7. You can also see how the maps become a focal point of collaboration and are constantly revised by the team to reflect current conditions and new ideas. This kind of continuous evaluation of the process as the design is progressing is increasing the quality and reliability of the information that is produced and is also helping to accelerate decision-making.

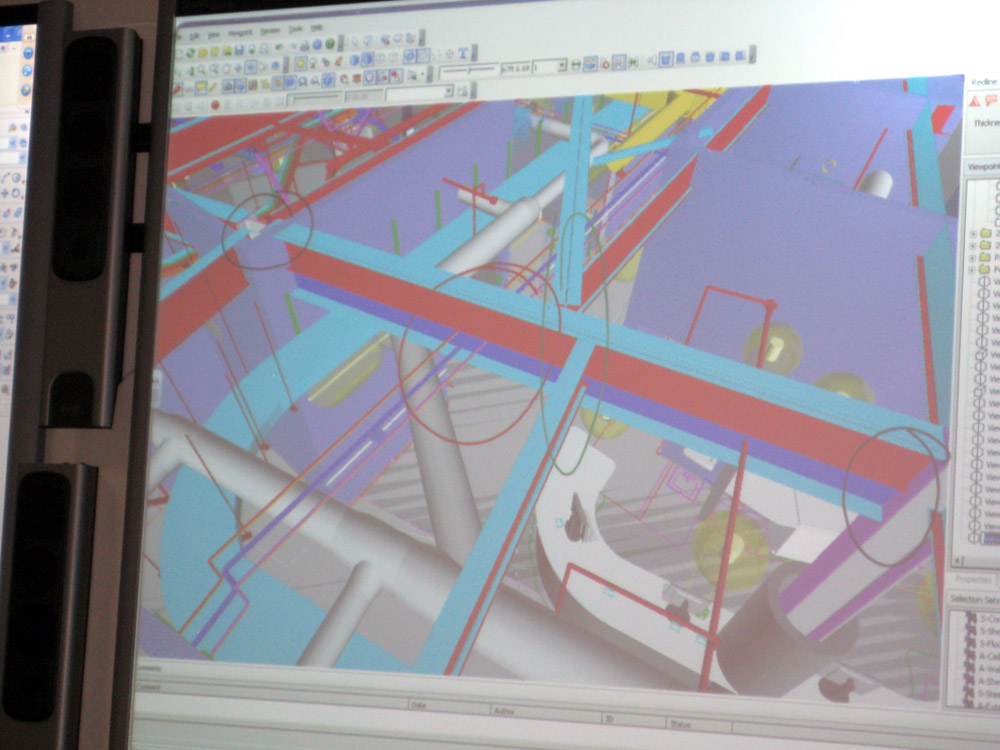
Face-to-face meetings has been one of the critical components of the IPD process for the SMCCV project, and a facility close to the site was rented specifically for this purpose. The entire project team has been meeting there at least biweekly, and those who cannot physically attend are remotely connected when required to the meeting sessions using the GoToMeeting collaboration application. I had the opportunity to attend one of these project meetings last month. The project was in the detailed design coordination phase, and the coordination process involved bringing all the individual disciplinary models into NavisWorks and reviewing them floor by floor. There were close to 30 people participating in the review process from the various disciplines and firms involved in the project, along with the representatives of the owner, Sutter Health. The model was projected on one large screen, with a second adjacent screen showing the related plan view, as shown in Figure 8. The project team was going over each room on the floor that was being reviewed that day, and exploring design aspects such as electrical, plumbing, ADA compliance, door swings, fire-rated walls, medical equipment, acoustics, lighting, and so on, asking questions and getting clarifications on issues from the specific team members responsible for them. The review process was primarily visual at this point and did not rely as much on the clash detection capabilities of NavisWorks, which are, however, being extensively used for other, more specific reviews such as detailed MEP routing.

Interestingly, on the day that I attended the SMCCV project meeting, a major issue surfaced, giving me the opportunity to witness first-hand how problems can be detected almost immediately in a collaborative design process and subsequently resolved, as opposed to the conventional process where changes can slip by un-noticed and end up creating major issues on the construction site. In reviewing the combined model within NavisWorks, the project team at one point detected some new beams that hadn’t originally been present, which were now clashing with some of the MEP ducts and conduits. There was a flurry of consternation and a “timeout” was declared to try and figure out what was going on. A NavisWorks capability that allows older and new versions of a model to be compared using color coding was used to determine exactly what had changed since the last review process (see Figure 9), and it turned out that in addition to the new beams that had been added, the depths of some of the existing beams had also been changed.
The members from the structural firm, TMAD, were not present at the meeting, but they were contacted right away, and remotely connected to the session using GoToMeeting. They acknowledged making changes in the design to address some loading issues caused by a skewed design condition. TMAD meets every two weeks with a third party reviewer to resolve comments on the structural package that they submitted to OSHPD in December. The reviewer disagreed with TMAD's solution to the skewed condition, and to ensure that the approval process stayed on track for a June permit, TMAD ran calculations and proposed a new solution—including some new beams and increasing the depth of some of the existing beams—that was in their mind the least impactful (least quantity length and size of beams) to the third party reviewer. Because they considered these as relatively minor modifications from a structural standpoint, they hadn’t informed the rest of the team about the changes. But the changes did cause problems elsewhere—in addition to the MEP clashes, there were some architectural issues as well. It was here that the power of online collaboration technology could really be appreciated—the speed with which the engineering team was connected remotely to the session, their ability to see the markups being added to the screen on which the model was projected, as well as being able to add markups themselves—it was almost as effective as being physically present there. Eventually, the issue with the structural changes was addressed by asking the engineers to work on resizing the new beams to make them as shallow as possible so that the clashes with other elements could be avoided. The issue has by now been fully resolved.
The most remarkable design metric for the SMCCV IPD project is that design time for structural was reduced from an expected 15 months to 8 months, and was informed by far more information from other disciplines than is usually available which led to better design quality. The other, more tentative, metric is that despite all the time spent planning the design process and meeting to do 3D coordination—all of which were billable hours—the cost for design is at or below what was anticipated. Thus, design is proceeding with higher quality, at a faster pace, and with no quantifiable increase in cost, at least up to this stage.
The SMCCV project can be considered as a landmark project in the US AEC industry as it is the first one to show that IPD is not just a utopian vision but a practical reality that can actually be implemented on large as well as small projects. First and foremost, though, it takes the initiative and leadership of an owner such as Sutter Health, which had the confidence to embark upon unchartered territory and put together a team that could actually deliver on this project as envisaged by the IPD concept. Having a dedicated consulting firm to manage the lean construction, BIM, and other technological aspects of the project has also helped greatly. The use of advanced technologies such as BIM and model-based collaboration and review has been critical to the IPD process, and it was extremely interesting to learn of the new technique of VSM and how it was used to streamline workflows and maximize efficiency. Last but not the least, credit has to go to the all the firms involved in this project, including the core IPD team as well as the larger project team. Their experience and willingness to adjust their traditional processes to take advantage of the opportunities of IPD has been the key to the success of this project so far.
At the same time, the incident with the unexpected structural changes that happened on the day I visited the project review meeting does highlight the fact that technology is no substitute for good communication. All of the participating firms learnt that individual team members should not make assumptions that their changes will not impact other disciplines, as they don’t know enough about what the others do. Any change made to the design causes a reactionary loop that can lead to other problems, which can be very expensive to fix later if they remain undetected. Even in the highly streamlined and collaborative SMCCV project workflow, one single incident of miscommunication caused the team to go through some additional design and review cycles. It was fortunate that the disruption turned out to be relatively minor, otherwise it would have been problematic for the tight design schedule.
Another key lesson learnt from the SMCCV project is the enormous benefit of face-to-face collaboration. Despite the availability of relatively advanced collaboration technologies such as online meeting applications and video conferencing, they do not seem to be an adequate substitute for coming together in the same room and working out design issues in real time. It seems that with IPD, the AEC industry is coming full circle—the profession that started out with a master builder, and subsequently went through enormous fragmentation over the years, is now bringing all those people back again together to design and construct better quality buildings more efficiently and effectively.
I would like to thank the entire SMCCV IPD team for hosting me at their project review meeting, giving me the opportunity to get a first-hand experience of the process. Special thanks also to Samir Emdanat of GHAFARI Associates for inviting me to study this project and supplying me with a lot of information about it, and to Digby Christian of Sutter Health and Bryan Johnson of Capital Engineering for taking the time to talk with me and provide their insights on the project.
Lachmi Khemlani is founder and editor of AECbytes. She has a Ph.D. in Architecture from UC Berkeley, specializing in intelligent building modeling, and consults and writes on AEC technology. She can be reached at lachmi@aecbytes.com.
AECbytes content should not be reproduced on any other website, blog, print publication, or newsletter without permission.